Intralesional glucocorticoid :
Used in Conditions like as follows :
-Dupuytren Contracture
-Gout in Renal Failure
-Keloids
-Alopecia areata
Intralesional glucocorticoid :
Used in Conditions like as follows :
-Dupuytren Contracture
-Gout in Renal Failure
-Keloids
-Alopecia areata
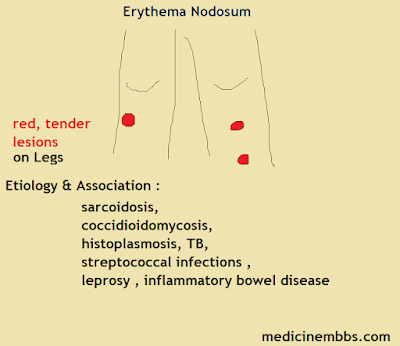
Sarcoidosis,
Coccidioidomycosis,
Histoplasmosis, TB,
Streptococcal infections,
Leprosy, inflammatory bowel disease
......... commonly used to prevent ischemic hypoxia brain injury out of hospital cardiac arrest?
Therapeutic hypothermia
Brain tumor with estrogen receptors?
meningioma
The hallmark of prolonged seizure and what the sequelae?
5 minutes...cortical laminar necrosis
Baby becomes floppy after family traveled to .............. or ................... or ......................?
California, Utah, Pennsylvania have been reported
BB, Primidone, topiramate, Deep brain stimulation or thalamotomy if all else fails
those are Treat for what?
essential tremor
1st line treatment in pseudotumor cerebri ?.
Rx: Acetazolamide ----> 1st line---> inhibit choroid plexus carbonic anhydrase↓ CSF and IH. Add
furosemide in pts with continued symptoms
Symptoms refractory to medical therapy or those
with progressive vision loss----> surgical intervention with optic nerve sheath decompression or
lumboperitoneal shunting is recommended.
Short-term use of corticosteroids or serial lumbar
puncture (LP) can serve as bridging therapy for patients awaiting definitive surgical treatment ---> not
recommended as primary intervention due to side effects
Subjective restlessness in a patient on antipsychotics...dx and RX?
Akathisia
beta-blocker ,benzodiazepine
Which artery is affected by Wallenberg syndrome?
PICA
We Add Dexamethasone in meningitis caused by what Bacterial infection?
Streptococcus pneumoniae and Haemophilus influenzae
MS symptoms last for how long Vs TIA symptoms?
For days and week vs less than 24 hours
In GBS what is the deep tendon reflex would be?
Dec or absent
Which Cranial nerve is responsible for Flavor perception?
cranial nerve VII
DTR that been seen in cyanide toxicity vs Magnesium Toxicity?
hyper vs hypo
Lyme meningitis is bacterial meningitis so what is WBC predominant?
lymphocytes
we Dx brain death clinically what is the criteria to Dx it?
absent cortical and brain stem functions. but, the spinal cord may still be functioning; therefore, deep tendon reflexes may be present.
Pulsus Tardus Parvus where do you see them?
AS
What is the BB that is CI in prolonged QT syndrome?
sotalol
MCC of erectile dysfunction post-infarction Patient ?
psychogenic
What causes the loss of the normal Right axis deviation in infants?
Tricuspid atresia
Quincke pulse where to see it ?
AR
what is the EKG looks like in Cardiac tamponade?
electrical alternans
1 - Exam that elicits pain for Tennis elbow?
Pain with resisted wrist extension and passive flexion
2 - Exam that elicits pain for Golfer's elbow?
Pain with resisted wrist flexion And with passive extension of the wrist
3 - Exam for De Quervain's tenosynovitis?
passive stretching of affected tendons ( passive ulnar deviation of the wrist ) by grasping flexed thumb into the palm with fingers elicits pain. (Finkelstein's test )
4 - Tendons affected in De Quervain's tenosynovitis?
Abductor Pollicious Longus and Extensor Pollicious Brevis
5 - Tendon affected/degenerated in tennis elbow?
Extensor Carpi Radialis Brevis
6 - What is Smith's Fx ? how did it happen?
Distal Radius Fx after falling on Flexed wrist, with anterior displacement of the distal part of the radius
7 - What is Colle's Fx? How did it happen?
distal radius Fx with posterior displacement of the distal part of radius and after fall on an outstretched hand
8 - Prophylaxis for Pseudo-gout ?
colchicine
9 - MCC of Osteomyelitis in SCD pt?
Salmonella
10 - Give 2 Orthopedic Conditions that are Negative Initially on X-ray.?
Scaphoid Fx and AVN
11 - MC location of Osteomyetlis in adults vs. Children?
vertebral body in adults Vs metaphysis of long bones in children
12 - Indication for X-ray in Low Back Pain?
Osteoprosis / compression Fx
Suspect Malignancy
A Spondylitis ( i.e Insidious onset, nocturnal, Pain better with movement )
13 - Indication For MRI in Low Back Pain Pt?
Sensory/ motor deficits
Cauda equina syndrome " urine retention Saddle anesthesia" Suspected epidural abscess /infection (e.g fever IV abuse concurrent infection, hemodialysis )
Abnormal initial X-Ray too
14 - Indication for CT scan in Low Back Pt?
Same Indication For MRI if Pt not able to do MRI
15 - We check what before hydroxychloroquine sulfate? how often do we check that?
baseline ophthalmic exam @ time of start Rx, then annually after 5 years
16 - Pain of Trochanteric bursitis elicited by?
Sleeping / Pressure on the affected Lateral side and Ext rotation and Resisted abduction
17 - MCC of Back pain?
Lumbosacral muscle strain
18 - Confirmatory test for carpal tunnel syndrome?
Nerve conduction study
19 - Exam to Dx Cong Hip Dysplasia?
Barlow and Ortolani
ultrasound after 2 weeks (not before) till 6 months, after six months we can do Xray.
20 - What maneuver to do to treat dislocation of the radial head?
Supination with Flexion Or hyperpronation of the elbow joint
21 - What Joints Spared in Rheumatoid Arthritis?
DIP and Sacroiliac lumbar, thoracic vertebrae
22 - What is Pathergy where to see it?
pustular skin lesions secondary to minor trauma
Behçet disease, Crohn's disease
23 - Skin finding in Reactive Arthritis?
Keratoderma blennorrhagicum & Circinate balanitis
24 - Risk F for Pseudogout ( associated with what Diseases )?
hemochromatosis and hyperparathyroidism hypothyroidism and DM and Wilson
25 - Risk F for torticollis ?
Risk factors Related to crowding in the uterus :
Multiple gestations, breach Position Oligohydrominous
26 - What Conditions/disease Related to intrauterine Position?
Metatarsal Adductus, Congenital Muscular torticollis CHD, and Club foot
27 - Neer test for?
Rotator cuff tendinopathy
28 - Pseudothrombophlibitis has been seen in?
bakers cyst rupture
29 - Hypertension Treatment in Pt with gout?
Losartan
30 - Which stress fracture needs to be treated with surgery?
Anterior tibial, 5th metatarsal
31 - Shin splints vs. tibial stress Fx?
shin splints are anterior leg pain in overweight pt who walk or run.
Vs
stress Fx is seen in underweight Pt and has localized pain.
32 - 2 cases we have to examine the neck before Anesthesia?
Rheumatoid Arthritis, Down Syndrome
33 - Rx of gout in Renal F Patient?
Intraarticular Steroid
34 - What is the most common stress fracture?
2nd metatarsal " March Fx "
35 - Which stress fracture needs to be treated with surgery?
Anterior tibial, 5th metatarsal
36 - Risk F for AVN?
Sickle cell
Caisson disease "decompression sickness"
Steroids
SLE,, steroid, antiphospholipid Antibodies syndrome "APLAS", alcohol,
37 - Nerve compressed in CTS Vs TTS?
Median N Vs Tibila N
38 - Staph Aureus tend to Affect Epiphysis T/F?
F Metaphysis
39 - Osteosarcoma Vs Ewing sarcoma Arise from?
Metaphysis vs diaphysis
40 - MCC of Acute prepatellar bursitis is?
Staph Aureus
41 - Anterior Ischemic Optic Neuropathy seen As A SE of Viagra? T/F
F we see it in GCA
42 - Drugs to avoid in myasthenia vs drugs to avoid in gout?
Aminoglycosides, BBs, Azithromycin, quinolones,
Vs
Thiazides and Aspirin.
43 - What is the site where giant cell tumors in the bone arises from?
Epiphysis
44 - What is Monteggia Fx ?
proximal 1/3 ulnar fracture with associated radial head dislocation/instability
45 - What is Galeazzi Fx ?
distal 1/3 radius shaft fx AND
associated distal radioulnar joint (DRUJ) injury
46 - What are the malignancy associated with dermatomyositis?
Ovarian, colon, pancreas lung stomach
47 - Medications Causing Drug-induced SLE with negative Anti histone?
Minocycline, Statin, Propylthiouracil
48 - What is the most accurate test to diagnose Sarcoidosis?
lymph node biopsy
49 - What is the treatment for renal osteodystrophy?
low phosphate diet, phosphate binders like sevelamer ( ca carbonate).Ca and vit D
50 - We provide CBT as Rx for Fibromyalgia T/F?
T
1. Which one is not a clinical presentation in Guillain Barre Syndrome?
Ascending paralysis
Weakness and paresthesias
Descending paralysis
Autonomic dysregulation
- C
2. CSF with an increased level of proteins +/- pleocytosis, and diffuse demyelination in nerve conduction studies are seen in:
Multiple Sclerosis
Amyotrophic Lateral Sclerosis
Myasthenia Gravis
Guillain-Barre Syndrome
- D
3. 40 yo man comes to the ED with progressive weakness and paresthesias in his legs, later in his arms over the last few days. In the Physical Exam is seen: SO2 90% (FiO2 21%), slightly dyspneic, lungs clear to auscultation bilaterally, Strength 3/5 in LE bilateral, 4/5 UE bilateral, areflexia in LE bilateral. The patient refers to an episode of diarrhea 3 weeks ago. What is the best initial step?:
IVIG infusion
Plasmapheresis
O2+ monitor Peak Inspiratory Pressure and Vital capacity
Nerve conduction studies
- C
4. 60 yo man presents with progressive swallowing impairment over the last 15 days, associated with weight loss. Also refers to weakness in his right hand later in his left hand that appeared 2 months ago. Denies pain, fever, night sweats, changes in bowel movements, urinary incontinence, paresthesias, tingling. PE fasciculations in tongue, weakness in UE and LE bilateral, atrophy in LE bilateral, Babinski + bilateral. Which of the following delay disease progression?
CPAP
Steroids
Plasmapheresis
Riluzole
- D
5. In the previous case, this medical condition is characterized for the following, except:
It is a progressive degenerative disease of both upper and lower motor neurons.
Associated with recent Campylobacter jejuni infection.
Paresthesias and autonomic dysregulation
B and C
- D
NEUROLOGY

1. Most common pathogen involved in Meningitis in Newborns group:
a) Listeria monocytogenes
b) Haemophilus influenzae
c) E. coli
d) Group B Streptococcus
D
2. Most common pathogen involved in Meningitis in teens group:
a) Haemophilus influenza
b) Streptococcus pneumonia
c) Neisseria meningitides
d) Enterovirus
C
3. Most common pathogen involved in Meningitis in adults:
a) Enterovirus
b) Neisseria meningitidis
c) Streptococcus pneumonia
d) Listeria monocytogenes
C
4. Most common pathogen involved in Meningitis in immunocompromised patients:
a) Herpes simplex virus
b) Cryptococcus spp.
c) Listeria monocytogenes
d) Gram negative bacilli
C
5. Best empiric treatment for Bacterial Meningitis in infants < 1 month and hyperbilirubinemia:
a) Vancomycin plus ampicillin plus Cefotaxime
b) Vancomycin plus ampicillin plus Ceftriaxone
c) Gentamicin plus ampicillin plus Cefotaxime
d) Gentaicin plus ampicillin plus Ceftriaxone
C
6. Best empiric treatment for Bacterial Meningitis in patients > 1 month to < 50 years:
a) Vancomycin plus ceftriaxone
b) Gentamicin plus ampicillin plus Cefotaxime
c) Gentamicin plus ampicillin plus Ceftriaxone
d) Vancomycin plus ampicillin
A
7. Best empiric treatment for Bacterial Meningitis in patients > 50 years:
a) Gentamicin plus ampicillin
b) Gentamicin plus ampicillin plus vancomycin
c) Vancomycin plus Cefotaxime
d) Vancomycin plus ampicillin plus ceftriaxone
D
8. Patient with contralateral weakness and sensory loss in the face and upper limbs PLUS hemispatial neglect. What is the affected artery?:
a) Anterior cerebral artery in the non-dominant hemisphere
b) Anterior cerebral artery in the dominant hemisphere
c) Middle cerebral artery in the non-dominant hemisphere
d) Middle cerebral artery in the dominant hemisphere
C
9. Patient with contralateral weakness and sensory loss in the face and upper limbs PLUS Broca’s aphasia PLUS right homonymous superior quadrantanopia. What is the most likely affected artery?
a) Left posterior cerebral artery
b) Right posterior cerebral artery
c) Right middle cerebral artery
d) Left middle cerebral artery
D
10. Patient with left hypoglossal palsy PLUS right hemiparesis AND right proprioception loss. What is the affected artery?:
a) Left paramedian branch of anterior spinal artery
b) Right paramedian branch of anterior spinal artery
c) Left superior cerebellar artery
d) Right anterior inferior cerebellar artery
A
11. The localization of lesion in Lateral medullary (Wallenberg) syndrome?:
a) Nucleus ambiguus, vestibular nuclei, lateral spinothalamic tract, and inferior cerebellar peduncle
b) Nucleus ambiguus, vestibular nuclei, lateral spinothalamic tract, and superior cerebellar peduncle
c) Nucleus ambiguus, vestibular nuclei, lateral corticospinal tract, and superior cerebellar peduncle
d) Nucleus ambiguus, vestibular nuclei, anterior corticospinal tract, and inferior cerebellar peduncle
A
12. Which artery is occluded in Lateral medullary (Wallenberg) syndrome?:
a) Anterior inferior cerebellar artery (AICA)
b) Posterior inferior cerebellar artery (PICA)
c) Superior cerebellar artery
d) Anterior spinal artery
B
13. Which condition is secondary to occlusion of the Basilar artery?:
a) Lateral pontine syndrome
b) Wallenberg syndrome
c) Dejerine syndrome
d) Locked-in syndrome
D
14. Patient with Lacunar infarcts. What are the affected artery and the risk factors associated with this patient’s condition?:
a) Lenticulostriate artery – Chronic hypertension and thoracic aortic aneurysm
b) Lenticulostriate artery – Chronic hypertension and abdominal aortic aneurysm
c) Middle cerebral artery - Chronic hypertension and thoracic aortic aneurysm
d) Middle cerebral artery - Chronic hypertension and abdominal aortic aneurysm
A

It is a neurodegenerative disease caused by prions
Accumulation in the brain of a normal protease-resistant prion protein
An elevated level of 14-3-3 protein in CSF
It is subacute dementia with rapid clinical progression
B
What is true about Huntington Disease?:
Life expectancy is 20 years from the time of diagnosis
Multiple abnormal CAG triplet repeats on chromosome 5
Anticipation is related to less severe disease
Multi9ple abnormal GAA triplet repeats on chromosome 9
A
Patient with Parkinson's Disease, his primary symptom is tremor. Which is the best medication?:
Amantadine
Benztropine
Selegiline
Entacapone
A
Mechanism of action of amantadine?:
A weak non-competitive NMDA receptor antagonist
It blocks the peripheral conversion of levodopa
Anticholinergic
MAO-B inhibitor
A
Mechanism of action of ropinirole and bromocriptine?:
MAO-B inhibitor
COMT inhibitor
Dopamine agonist
Anticholinergic
C
Mechanism of action of Selegiline?:
Anticholinergic
COMT inhibitor
Dopamine agonist
MAO-B inhibitor
D
Mechanism of action of Entacapone and tolcapone?:
Anticholinergic
COMT inhibitor
Dopamine agonist
MAO-B inhibitor
B
Mechanism of action of Benztropine and trihexyphenidyl?:
Anticholinergic
COMT inhibitor
Dopamine agonist
MAO-B inhibitor
A
What is the most often primary cancer in metastatic brain tumors?:
Breast cancer
GI tract cancer
Melanoma
Lung cancer
D
Symptoms of increased intracranial pressure?:
Nausea, vomiting, headache, and confusion
Nausea, vomiting, headache, and diplopia
Fever, weight loss, and headache
Headache, fever, and nuchal rigidity
B
Diagnostic criteria for Neurofibromatosis 1, except:
Café-au-lait spots
Optic glioma
Lisch nodules
Bilateral vestibular schwannomas
D
Patient with a history of Meningioma and neurofibroma. What is the diagnosis?:
Neurofibromatosis 1
Neurofibromatosis 2
Tuberous Sclerosis
Sturge-Weber disease
B
What structures are included in the limbic system?:
Caudate, putamen, globus pallidus, substantia nigra, and subthalamic nucleus
Habenula, habenular commissure, posterior commissure, and the pineal gland
Subthalamic nucleus, red nucleus, and substantia nigra
Amygdala, hippocampus, fornix, mammillary bodies, cingulate gyrus, and parahippocampal gyrus
D
What structures are included in Basal ganglia?:
Caudate, putamen, globus pallidus, substantia nigra, and subthalamic nucleus
Habenula, habenular commissure, posterior commissure, and the pineal gland
Subthalamic nucleus, red nucleus, and substantia nigra
Amygdala, hippocampus, fornix, mammillary bodies, cingulate gyrus, and parahippocampal gyrus
A
What structures are included in the Epithalamus?:
Caudate, putamen, globus pallidus, substantia nigra, and subthalamic nucleus
Habenula, habenular commissure, posterior commissure, and the pineal gland
Subthalamic nucleus, red nucleus, and substantia nigra
Amygdala, hippocampus, fornix, mammillary bodies, cingulate gyrus, and parahippocampal gyrus
B
What structures are included in the Subthalamus?:
Caudate, putamen, globus pallidus, substantia nigra, and subthalamic nucleus
Habenula, habenular commissure, posterior commissure, and the pineal gland
Subthalamic nucleus, red nucleus, and substantia nigra
Amygdala, hippocampus, fornix, mammillary bodies, cingulate gyrus, and parahippocampal gyrus
C
Pathway in Papez circuit?:
Fornix hippocampus mammillary bodies mammillothalamic tract anterior nucleus of the thalamus thalamocingulate radiation cingulate gyrus hippocampus
Hippocampus mammillary bodies fornix mammillothalamic tract anterior nucleus of the thalamus thalamocingulate radiation cingulate gyrus hippocampus
Hippocampus fornix mammillary bodies mammillothalamic tract anterior nucleus of the thalamus thalamocingulate radiation cingulate gyrus hippocampus
Hippocampus fornix mammillary bodies mammillothalamic tract anterior nucleus of the thalamus cingulate gyrus thalamocingulate radiation hippocampus
C
What is the function of the ventromedial nucleus?:
Satiety
Hunger
Heat dissipating
Heat conservation
A
What is the function of the anterior hypothalamus?:
Satiety
Hunger
Heat dissipating
Heat conservation
C
What is the function of the posterior hypothalamus?:
Satiety
Hunger
Heat dissipating
Heat conservation
D
What is the function of the lateral area of the hypothalamus?:
Satiety
Hunger
Heat dissipating
Heat conservation
B
What is the function of suprachiasmatic nuclei?:
Heat conservation
Heat dissipating
Circadian rhythms
Synthesis of vasopressin and oxytocin
C
What is the function of supraoptic and paraventricular nuclei?:
Heat conservation
Heat dissipating
Circadian rhythms
Synthesis of vasopressin and oxytocin
D
The classic triad of Wernicke encephalopathy?:
Encephalopathy, ophthalmoplegia, and ataxia
Encephalopathy, ophthalmoplegia, and anterograde amnesia
Encephalopathy, ophthalmoplegia, and retrograde amnesia
Encephalopathy, horizontal nystagmus, and confabulations
A
Signs and symptoms of Korsakoff dementia?:
Encephalopathy, ophthalmoplegia, and ataxia
Encephalopathy, ophthalmoplegia, ataxia, amnesia, and confabulations
Encephalopathy, ophthalmoplegia, ataxia, and tremor
Encephalopathy, ophthalmoplegia, ataxia, and paraplegia
B
Which vitamin deficiency causes Wernicke encephalopathy?:
Vitamin B12
Vitamin B9
Vitamin B3
Vitamin B1
D
Which vitamin deficiency causes peripheral neuropathy?:
Vitamin B12
Vitamin B9
Vitamin B3
Vitamin B1
A
What is the etiology of Closed-Angle Glaucoma?:
Obstruction of drainage pathways by the iris
Decreased drainage due to damaged trabecular meshwork
Macular degeneration
Retinal vascular occlusion
A
What is the etiology of Open-Angle Glaucoma?:
Obstruction of drainage pathways by the iris
Decreased drainage due to damaged trabecular meshwork
Macular degeneration
Retinal vascular occlusion
B
Treatment for Open-Angle Glaucoma?:
Isoproterenol
Timolol
Furosemide
Atropine
B
The lesion in the left optic nerve and defect in the visual field?:
Right anopia
Right homonymous hemianopsia
Left homonymous hemianopsia
Left anopia
D
The lesion in the optic chiasm and defect in visual field?:
Central scotoma
Left hemianopia with macular sparing
Bitemporal hemianopsia
Right homonymous hemianopsia
C
The lesion in the right optic tract and defect in visual field?:
Right homonymous hemianopsia
Left homonymous hemianopsia
Left lower quadrantic anopsia
Right lower quadrantic anopsia
B
The lesion in left dorsal optic radiation?:
Right lower quadrantic anopsia
Left lower quadrant anopsia
Right upper quadrantic anopsia
Left upper quadrantic anopsia
A
The lesion in right Meyer Loop and defect in the visual field?:
Right lower quadrantic anopsia
Left lower quadrant anopsia
Right upper quadrantic anopsia
Left upper quadrantic anopsia
D
Left PCA infarction and defect in the visual field?:
Left hemianopsia with macular sparing
Right hemianopsia with macular sparing
left lower quadrantic anopsia
right lower quadrantic anopsia
B
Macular degeneration and defect in visual field?:
Hemianopsia with macular sparing
Upper quadrantic anopsia
Lower quadrantic anopsia
Central scotoma
D
What is true about central retinal artery occlusion?:
Swollen optic disc with hemorrhages
Retinal hemorrhages
Cotton-wool spots
Cherry-red spot of the fovea
D
What is true about central retinal vein occlusion?:
Retinal swelling
Bloodless retinal arteries
Cotton-wool spots
Cherry-red spot
C
HEMATOLOGY
Most common coagulation disorder in Ashkenazi Jews?:
Hemophilia A
Hemophilia B
Hemophilia C
Von Willebrand Disease
C
Mechanism of action of Heparin?:
Inhibits synthesis of vitamin K-dependent coagulation factors
Directly inhibit factor Xa
Inhibits factor II
Activates antithrombin
D
Mechanism of action of Warfarin?:
Inhibits synthesis of vitamin K-dependent coagulation factors
Directly inhibit factor Xa
Inhibits factor II
Activates antithrombin
A
Mechanism of action of Apixaban?:
Inhibits synthesis of vitamin K-dependent coagulation factors
Directly inhibit factor Xa
Inhibits factor II
Activates antithrombin
B
Mechanism of action of Dabigatran?:
Inhibits synthesis of vitamin K-dependent coagulation factors
Directly inhibit factor Xa
Inhibits factor II
Activates antithrombin
D
Mechanism of action of tPA?:
Inhibits synthesis of vitamin K-dependent coagulation factors
Directly inhibit factor Xa
Converts plasminogen into plasmin which breaks down fibrin
Activates antithrombin
C
The best initial test in the diagnosis of Hemophilia?
PTT
Mixing study
Specific factor assays
PT
B
Most accurate test in the diagnosis of Hemophilia?:
PTT
Mixing study
Specific factor assays
PT
C
What is the most common inherited bleeding disorder?:
Von Willebrand Disease
Hemophilia A
Bernard-Soulier syndrome
Glanzmann thrombasthenia
A
What is the most common cause of hereditary thromboembolic disease?:
Antithrombin III deficiency
Protein C deficiency
Factor V Leiden
Protein S deficiency
C
In which condition is seen decreased agglutination on the ristocetin cofactor assay?
Factor V Leiden
Von Willebrand disease
Bernard-Soullier syndrome
Glanzmann thrombasthenia
B
What is the condition caused by a deficiency in GpIIb/IIIa?:
Factor V Leiden
Von Willebrand disease
Bernard-Soullier syndrome
Glanzmann thrombasthenia
D
What is the condition caused by a deficiency in GpIb?:
Factor V Leiden
Von Willebrand disease
Bernard-Soullier syndrome
Glanzmann thrombasthenia
C
What is the mechanism of action of Clopidogrel and ticlopidine?:
Inhibits ADP receptor
Inhibits GpIIb/IIIa
Inhibits COX
Inhibits factor II
A
Lab findings in Von Willebrand disease?:
Increased bleeding time
Decreased PTT
Increased PT
Decreased platelet count
A
What is the cause of Idiopathic thrombocytopenic purpura?:
Deficiency of ADAMTS-13
IgG antibodies against patient’s platelets
Depletion of clotting factors and platelets
PF4 antibody
B
What is the cause of Thrombotic Thrombocytopenic Purpura?:
Deficiency of ADAMTS-13
IgG antibodies against patient’s platelets
Depletion of clotting factors and platelets
PF4 antibody
A
What is the cause of Heparin-induced Thrombocytopenia?:
Deficiency of ADAMTS-13
IgG antibodies against patient’s platelets
Depletion of clotting factors and platelets
PF4 antibody
D
What is the cause of tissue necrosis following warfarin administration?:
Vitamin C and S deficiency
Vitamin K deficiency
Activation of protein C
Activation of protein S
A
Clinical presentation and lab findings in TTP?:
Hemolytic anemia increased creatinine and low platelets without neurologic symptoms
Hemolytic anemia increased creatinine, low platelets, increased TP, increased bleeding time
Hemolytic anemia, increased creatinine, low platelets, seizure, and fever
Hemolytic anemia, increased creatinine, low platelets, retroperitoneal bleeding, and fever
C
Clinical presentation and lab findings in HUS?:
Hemolytic anemia increased creatinine, and low platelets without neurologic symptoms
Hemolytic anemia increased creatinine, low platelets, increased TP, increased bleeding time
Hemolytic anemia, increased creatinine, low platelets, seizure, and fever
Hemolytic anemia, increased creatinine, low platelets, retroperitoneal bleeding, and fever
A
Best initial abortive therapy for Migraine?:
Gabapentin
Triptans
NSAIDs
Dihydroergotamine
C
Prophylaxis for Migraine includes, except:
a) Propanolol
b) Amitriptyline
c) Triptans
d) Topiramate
C
Best initial abortive therapy for Cluster headaches?:
a) 100% O2
b) NSAIDs
c) Triptans
d) Acetaminophen
A
Best prophylactic therapy for Cluster headache?:
a) Valproate
b) Propanolol
c) Amitriptyline
d) Verapamil
D
A 34-year-old patient presents with severe, shooting pain, 6/10, on the right side of his face. It lasts less than one minute and presents several times during the day. He states the pain is worse after chewing or brushing his teeth. He denies fever, changes in his vision, lacrimation, rhinorrhea, nausea, or vomiting. What is the best explanation for his condition?:
a) Migraine
b) Trigeminal neuralgia
c) Cluster headache
d) Temporal arteritis
B
What is the first-line therapy for the condition of the previous patient?:
a) Verapamil
b) Valproate
c) Carbamazepine
d) Steroids
C
37-year-old female patient presents to ED for severe, constant, pressure-like headache (worst pain of my life), 10/10, that started suddenly this morning while she was exercising. The pain is getting worse, doesn’t alleviate with anything. It is associated with nausea, vomiting, photophobia. The physical exam is remarkable for the presence of the Brudzinski sign. What is the best initial step?:
a) Lumbar puncture and CSF analysis
b) CT scan of the head without contrast
c) CT scan of the head with contrast
d) MRI brain
B
First-line therapy in children with partial or tonic-clonic seizures?:
a) Levetiracetam
b) Phenytoin
c) Carbamazepine
d) Phenobarbital
D
First-line therapy for Absence seizures?:
a) Valproic acid
b) Levetiracetam
c) Ethosuximide
d) Carbamazepine
C
Which is the best initial therapy in status epilepticus?:
a) Midazolam
b) Phenytoin
c) Phenobarbital
d) Lorazepam
D
A patient is still in status epilepticus after 20 minutes besides the administration of benzodiazepines every 5 minutes, which is the best next step?:
a) Continue benzodiazepine for 20 more minutes
b) Start Phenytoin
c) Start Fosphenytoin
d) Start Phenobarbital
C
When is recommended continuous EEG monitoring?:
a) In convulsive status epilepticus
b) Patient does not wake up after clinically obviously seizures stop
c) During alcohol withdrawal
d) During benzodiazepines withdrawal
B
A 55-year-old patient presents in ED with sudden severe vertigo, nausea, vomiting, and difficulty standing up. He was diagnosed with URI 10 days ago. The physical exam is remarkable for vertical nystagmus and gait unsteadiness. He has a past history of Hypertension, DM T1, and CHF. What is the best initial step?:
a) Diffusion-weighted MRI
b) Start meclizine
c) Start steroids
d) Start NSAIDs
A
In the presentation of Benign Paroxysmal Positional Vertigo, which one is incorrect?:
a) Vertigo lasts < 1 min
b) It is not associated with hearing loss
c) Epley maneuver can resolve the symptoms
d) Meclizine is the best initial therapy
D
In Labyrinthitis, which of the following symptoms is incorrect?:
a) Lacking hearing loss
b) Tinnitus
c) Ear fullness
d) Nausea and vomiting
A
What is correct about Ménière's disease?:
a) Recurrent episodes of vertigo, tinnitus, nausea, vomiting, and hearing loss
b) Acute vertigo, nausea, vomiting, and hearing loss after a recent URI
c) Acute vertigo and nystagmus triggered by changes in head position
d) Acute vertigo, nausea, vomiting without hearing loss after a recent URI
A
What is correct about Vestibular neuritis?:
a) Recurrent episodes of vertigo, tinnitus, nausea, vomiting, and hearing loss
b) Acute vertigo, nausea, vomiting, and hearing loss after a recent URI
c) Acute vertigo and nystagmus triggered by changes in head position
d) Acute vertigo, nausea, vomiting without hearing loss after a recent URI
D
Lab findings in Iron Deficiency Anemia?:
High ferritin, high RDW, high TIBC, low serum iron
Low ferritin, low RDW, high TIBC, low serum iron
Low ferritin, high RDW, high TIBC, low serum iron
Low ferritin, low RDW, low TIBC, low serum iron
C
Lab findings in Anemia of Chronic Disease?:
High ferritin, low serum iron, normocytic anemia
Low ferritin, low serum iron, microcytic anemia
High ferritin, high serum iron, normocytic anemia
Low ferritin, high serum iron, normocytic anemia
A
Lab findings in Megaloblastic Anemia due to B12 deficiency?:
Macrocytic anemia increased MMA and increased homocysteine
Macrocytic anemia, normal MMA, and increased homocysteine
Macrocytic anemia, normal MM, and normal homocysteine
Macrocytic anemia, increased MMA, and normal homocysteine
A
Lab findings in Megaloblastic Anemia due to B9 deficiency?:
Macrocytic anemia increased MMA and increased homocysteine
Macrocytic anemia, normal MMA, and increased homocysteine
Macrocytic anemia, normal MM, and normal homocysteine
Macrocytic anemia, increased MMA, and normal homocysteine
B
What is the most common cause of osteomyelitis in patients with Sickle Cell Disease?:
S aureus
Salmonella
S epidermidis
Shigella
B
What is false about complications in Sickle Cell Disease?:
Splenic sequestration resulting in hypovolemia
Parvovirus B 19 infection resulting in aplastic crisis
Low platelets
Increased PTT
D
What is true about Warm Autoimmune Hemolytic Anemia?:
Presence of IgM antibodies
Presence of IgG antibodies
It is associated with Mycoplasma pneumonia
It is associated with Mononucleosis
B
What is true about Cold Autoimmune Hemolytic Anemia?:
Presence of IgG antibodies to RBC antigens
It is associated with Mycoplasma pneumonia
It is associated with Mononucleosis
It is associated with SLE
D
All are true about Hereditary spherocytosis, except?:
Presence of spherocyte
Positive osmotic fragility tests
Negative direct Coombs test
Positive direct Coombs test
D
What is not a cause of Aplastic Anemia?:
HIV infection
Parvovirus B 19 infection
Sulfa drugs
Ciprofloxacin
D
What is not true about Thalassemia?:
African, Middle Eastern, and Asian descent are mostly affected
Microcytic anemia with normal serum iron
Microcytic anemia with low serum iron
Most patients with Thalassemia do not require treatment
C
What is not present in hyperviscosity syndrome ?:
Easy bruising
Blurred vision
Pruritus after a cold bath
Thrombosis
C
What is the best initial test in the diagnosis of Polycythemia Vera?:
JAK 2 mutation
CBC
CBC with an ABG and EPO level
EPO levels
C

